Advanced Therapy Medicinal Products (ATMPs) are human medicines based on cells, genes, or tissues and are seen as pioneering new opportunities for the treatment of a range of diseases. Currently, 22 ATMPs have been approved by the FDA, and the field of interest is growing rapidly. In traditional drug development, pharmacokinetic (PK) studies are necessary to use medicines under the best conditions of efficacy and safety.
For ATMPs, investigations of PK are also essential aspects as delineated in EMA’s guide on ATMPs, including flowcharts and checklists. However, there could be significant differences compared to traditional ADME (Absorption, Distribution, Metabolism, and Excretion) studies, and special considerations unique to the respective ATMPs are required. This is because ATMPs may not follow the common principles of ADME or exhibit a classical dose-response relationship. For example, in the case of cell therapies, clinical PK studies may consider body distribution/migration, cells growth, viability, differentiation/proliferation, and/or phenotype, depending on what is relevant to the specific ATMP.
Among 22 ATMPs approved by the FDA, five are chimeric antigen receptors (CAR) T-cell therapies: tisagenlecleucel (Kymriah™), lisocabtagene maraleucel (Breyanzi®), axicabtagene ciloleucel (Yescarta ™), idecabtagene vicleucel (Abecma®), and brexucabtagene autoleucel (Tecartus™). In this blog, we shed light on CAR-T therapy as an example case for ATMP drug development.
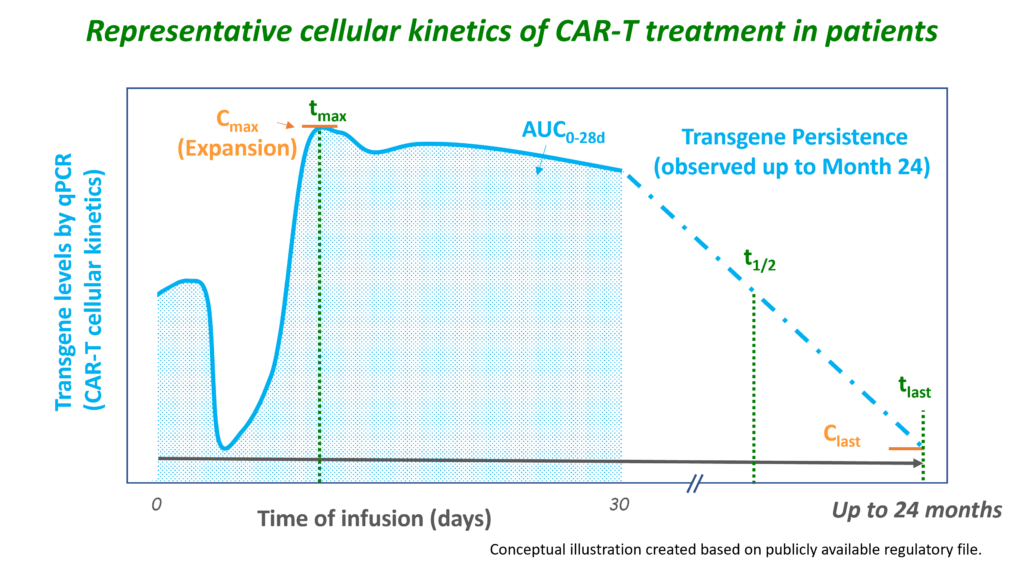
CAR-T therapy involves genetically engineering and expanding autologous (or, in the future, potentially allogeneic) T-cells, after which the modified T-cells are administered to the patient. The genetically engineered CAR-T cells are adapted to target tumour cells using the CAR, which binds to specific antigens on tumour cells. After infusion, the concentration of CAR-T cells observed in the blood declines as the CAR-T cells distribute into the tissues. Upon interaction with the tumour target, the CAR-T cells become activated and rapidly expand, which can be measured as a rise to maximum concentrations in the blood (1-2 weeks after infusion). After this peak, the concentrations slowly decline, reflecting the death of the CAR-T cells (e.g. due to a decrease in tumour burden). However, CAR-T cell concentrations may continue to be observed for years and can even increase again when available target tumour cells increase. Since the engineered CAR gene is directly related to the expansion and persistence of CAR-T cells, PK studies are necessary in the development of these ATMPs.
Therefore, unlike most ATMP products, the PK of CAR-T cells involves the evaluation of traditional ADME PK parameters, but these need to be interpreted in the context of cellular kinetic parameters indicative of expansion (Cmax) and persistence (AUC, tlast). At Venn Life Sciences, our team of experienced consultants and data analysts has the expertise to support and manage PK analyses for new therapies like ATMPs.
The PK profiles of CAR-T cells do not always reflect a traditional PK profile, and therefore the following practical aspects need to be taken into account:
If you are interested in learning more about how we can support you with PK in ATMPs, please contact Venn Life Sciences at BD@vennlifesciences.com. We would welcome the opportunity to discuss PK in ATMPs and other related aspects.



